One of the most important ways we can reduce the incidence of suicide is become more willing to talk about mental illness. If people are identified early, before their illnesses get so severe, they may respond to treatment and this whole post might be unnecessary in their case.
We need our communities to become places where it is considered normal to ask people questions like:
- How have you been feeling in your mood recently?
- What has been on your mind lately?
- Does anyone think that you something that you have said is odd or unusual?
- Are you sleeping OK?
- Are you eating OK?
- How are your stress levels?
- Are you able to get things done, or is it all getting a bit much?
- Have you had any unusual experiences lately?
- Are you hopeful about the future?
We can all play our part in screening for mental illness and encouraging people to reach out for professional help.
Help When Life Hurts
This article is part of a growing collection, drawing from Adrian Warnock’s medical and psychological expertise, lived experience, and Christian faith.
Click the type of pain you or a loved one are experiencing right now
General suffering & disappointment
Financial difficulties
Feeling disqualified
Chronic illness & disability
Divorce & family pain
Depression & mental health
Bereavement & end-of-life
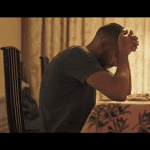
But we need to go a step future too. Mental illnesses will be associated in some people with Suicidal thoughts or acts. It is vital to appreciate that at points during their illnesses some patients will pose a threat to their own safety, or even (much more rarely) the safety of others. One thing that all pastors, and Christians who want to care need to learn is how to sensitively address this issue.
Some people are afraid of asking someone a question like, “Have you ever wished you were dead or wished you could go to sleep and not wake up?” One concern is that asking the question might prompt the act. But, provided it is done sensitively there is no evidence to support that fear. On the contrary, simply discussing the dark thoughts with another caring person can sometimes alleviate them. There is no doubt that asking such a question during pastoral care, or even a conversation between friends can save lives.
I am not at this point proposing it should be asked in every single pastoral interaction, as clearly it needs to be appropriately framed. If, for example, a couple came to you asking for pastoral counseling about their recent engagement, it might be a bit odd to ask them if they were suicidal. But the question could definitely be asked whenever someone appears distressed, hopeless, or in any sense desperate for help. Of course, some people are very good at hiding their distress. If a person visiting with you seems like they have something they want to talk about but appear not ready to speak, asking this question could open them up, even if the answer is “Oh no, pastor, it hasn’t got that bad!”
If you ask this question and the answer is “yes,” don’t panic. First, ask them “When did you feel like this?” They may reply, “Twenty years ago, once.” The timing is critical. If the thoughts are current, it is really the time for a non-expert to hand over the case to an expert assessment. It is often not inappropriate, however, to briefly explore a little further, and the next question would be “have you had any actual thoughts of killing yourself?”
The CSSRS is a suicide assessment scale used by professionals. You should not try and second-guess an expert in mental illness, but a review of the scale’s risk factors, and the questions used will help you gain at least a basic understanding of how psychiatrists view the risk of self harm. Training is available in the use of this scale for non-psychiatrists.
There are several levels of risk, and again, you are probably not best placed to determine for sure where to put someone on that list, but I will give you the broad outlines anyway:
- The general wish to be dead without any thoughts of harming yourself (this should still be taken seriously, but is a lower risk than the other levels).
- The presence of thoughts to kill yourself without any thoughts of how you might kill yourself.
- The presence of a method This is a general idea only, without specific details or any wish to actually carry it out, i.e the thoughts may feel quite alien to the person.
- The presence of some intent to actually kill yourself, but without specific plans.
- The presence of a detailed plan with methods, timing, and some form of plan to carry it out.
Of course, any actual suicidal act is especially concerning, and will definitely require immediate assessment of a person by a psychiatrist. Even “cutting” or other self-harm acts can be indicative of a very serious underlying problem.
I haven’t gone into much detail about harm to others, but clearly a similar principle applies. If you are concerned a person has ideas about harming themselves or others it is not the time to call a prayer meeting. First, get the patient assessed by a professional. At this point it really doesn’t matter whether that expert shares your faith or not.
Don’t attempt to handle all this informally within a church. Far better to take someone in for an assessment and be told that the doctor believes they are fine than to not act. By all means pray once the person has been taken to hospital, or get a group to pray while that is happening.
Even before such a situation happens, I would urge every pastor to become familiar with how to access urgent psychiatric help in their area. Why not reach out to local services, and ask for their advice how you can best serve church members who may have mental illness. There may even be a need for a local drop-in service which perhaps you could help them with.
There are procedures in most countries for getting an at-risk person assessed even against their wishes. Find out how to request that before you are facing the situation. If you are unsure, a primary care physician (GP in the UK) is likely to be able to help you understand the appropriate steps to take.
People can also be referred to suicide prevention helplines like The National Suicide Prevention Helpline in the USA, and The Samaritans in the UK. Both organizations are willing to take a call from a friend, family member or pastor, and have advice pages for those who are concerned about someone (see the USA and UK pages). Speaking on the phone on its own should not take the place of getting a face-to-face professional assessment.
There are other things that are important including reducing access to means of suicide. Society as a whole can do a better job of making it hard to get ahold of ways to kill yourself. There is lots of evidence that suicide is usually an impulsive act, and an attempt will not always be repeated if it is aborted because the method is not available or turns out not to be deadly. This is one of the strongest arguments for gun control. Suicides were reduced by a change in the form of gas pumped to peoples homes, and governments often consider other means of making popular methods obsolete.
There are some things that friends and families can do to restrict someone’s access to ways to harm themselves. But, if you are finding that you have become an informal policeman, this is not sustainable, and the time has definitely come to seek professional help.
Even with the best of care, not every suicide is preventable. It is impossible to reduce the risk to zero while we live in a free society. There is no doubt that dealing with potential and actual suicides is one of the hardest things friends, family and pastors have to face.
I hope this post has been helpful, and now it is over to you. Are there any other useful resources or tips you would like to share with my readers?

 → What does Jesus’ resurrection mean for you?
→ What does Jesus’ resurrection mean for you?
 → Why is change so difficult? What causes the resistance?
→ Why is change so difficult? What causes the resistance?
 →
Why is change so slow? How does grace lead us over a lifetime?
→
Why is change so slow? How does grace lead us over a lifetime?
 →
How do you become a Christian? How do you know if you really are one?
Hope Reborn: How to Become a Christian and Live for Jesus
→
How do you become a Christian? How do you know if you really are one?
Hope Reborn: How to Become a Christian and Live for Jesus